THE SILENT EPIDEMIC NOBODY TALKS ABOUT
In 2019, the CDC published data showing that only 12% of US adults have optimal metabolic health — defined as healthy levels of blood sugar, blood pressure, cholesterol, triglycerides, and waist circumference, without medication.
That means 88% of American adults have at least one metabolic problem. Many have several. And the majority of those people look and feel roughly normal — at least for now.
Insulin resistance is one of the earliest and most common drivers of metabolic dysfunction. It develops silently over years, rarely causing obvious symptoms until it has progressed to prediabetes or type 2 diabetes. By the time most people find out they have it, it's already been affecting their health for a decade.
The blunt question is: are you one of the 88%? And the blunter follow-up: do you have any idea?
Personal take
I was never slim — overweight from childhood, every year of it. My grandparents survived wartime scarcity and channelled that experience into feeding everyone around them with unconditional generosity; it worked on me. Now that longevity has become a real concern rather than a distant concept, I went deeper into the metabolic research. What surprised me was how strongly visceral fat predicts insulin resistance risk, even after accounting for overall body weight. That sent me straight to a tape measure.
88%
of US adults have at least one marker of metabolic dysfunction
Source: Araújo et al., Metabolic Syndrome and Related Disorders, 2019
Personal take
That number isn't abstract for me. When I built this tool, I ran my own numbers and came up in the red. I have non-alcoholic fatty liver disease — a condition that goes hand in hand with visceral fat accumulation and metabolic dysfunction. My blood work doesn't show insulin resistance yet, but my values sit in the upper range. That's exactly the range where things are still reversible. Which is part of why I built this.
Curious where you fall?
Enter your height and waist circumference. Takes 30 seconds. No blood draw. No sign-up.
Check my risk →WHAT INSULIN RESISTANCE ACTUALLY IS
Insulin is a hormone produced by the pancreas. Its job is to escort glucose (sugar) from your bloodstream into your cells, where it's used for energy. In a healthy system, a small amount of insulin clears blood sugar quickly and efficiently.
Insulin resistance is when that system starts failing. Your cells stop responding normally to insulin signals. To compensate, your pancreas secretes more insulin to get the same job done. Blood sugar stays elevated longer after meals. The pancreas works harder and harder.
Over time, this leads to:
- Prediabetes (chronically elevated blood sugar below the diabetes threshold)
- Type 2 diabetes (pancreas can no longer keep up)
- Elevated triglycerides and reduced HDL cholesterol
- Higher risk of cardiovascular disease
- Non-alcoholic fatty liver disease (NAFLD)
- Polycystic ovary syndrome (PCOS) in women
These are not distant outcomes. They develop gradually — while blood sugar readings stay normal and routine checkups find nothing to flag. In many people, insulin resistance begins years before fasting glucose becomes abnormal. By the time blood sugar rises, the underlying process may have been developing for a long time.
The underlying driver is almost always the same: excess visceral fat — fat stored inside the abdominal cavity, wrapped around your organs. Visceral fat secretes inflammatory compounds and fatty acids that directly interfere with insulin signaling.
"Visceral fat is the dangerous kind — and it's invisible on the outside. Your waist-to-height ratio is the closest thing to an X-ray you can do at home."
WHY INSULIN RESISTANCE OFTEN GOES UNDETECTED
Standard blood panels check fasting glucose. If your fasting glucose is under 100 mg/dL, you're told you're fine. But this misses the problem entirely.
Fasting glucose stays normal for years while insulin resistance develops. In many people, fasting insulin rises long before fasting glucose becomes abnormal — the pancreas working harder to compensate. But fasting insulin is not included in standard metabolic panels in most routine checkups. It requires a separate order, and many doctors don't think to ask for it unless you're already showing signs of diabetes.
By the time your fasting glucose is elevated — which is the standard trigger for diagnosis — you may have had insulin resistance for 5–15 years.
This is why proxy measures matter. You can't easily measure your insulin at home, but you can measure your waist circumference. And your waist-to-height ratio turns out to be a surprisingly reliable proxy for the visceral fat that drives insulin resistance.
WAIST-TO-HEIGHT RATIO: THE MEASUREMENT THAT MATTERS
Waist-to-height ratio (WHtR) is exactly what it sounds like: your waist circumference divided by your height, both in the same unit.
WHtR = waist circumference ÷ height
A person who is 180 cm tall with a 90 cm waist has a WHtR of 0.50. The same person with a 100 cm waist has a WHtR of 0.56.
The key threshold is 0.5 — your waist should be less than half your height. This boundary was derived from large population studies and has been validated in dozens of research efforts totaling hundreds of thousands of participants.
WHtR risk categories
| WHtR | Category | Metabolic risk |
|---|---|---|
| Below 0.40 | Very lean | Lowest risk |
| 0.40 – 0.49 | Healthy range | Low risk |
| 0.50 – 0.59 | Elevated | Moderate risk |
| 0.60 or above | High | High risk |
Why WHtR beats BMI
BMI is a ratio of weight to height squared. It has two major flaws as a metabolic health indicator:
- It doesn't distinguish muscle from fat. A muscular person and an obese person can have identical BMIs.
- It ignores fat distribution. A person with a large waist and thin legs has very different health risks than a person with the same weight distributed more evenly — and BMI treats them identically.
WHtR directly measures central adiposity — where the metabolically dangerous fat accumulates. Multiple meta-analyses have confirmed that WHtR outperforms BMI as a predictor of cardiometabolic risk, type 2 diabetes, and all-cause mortality.
It also has a universal threshold. The 0.5 boundary doesn't vary meaningfully by sex — unlike waist-to-hip ratio, which requires different reference ranges for men and women.
HOW TO USE INRESRISK
InResRisk takes two inputs: your waist circumference and your height. That's it. No sign-up. No account. No blood test required.
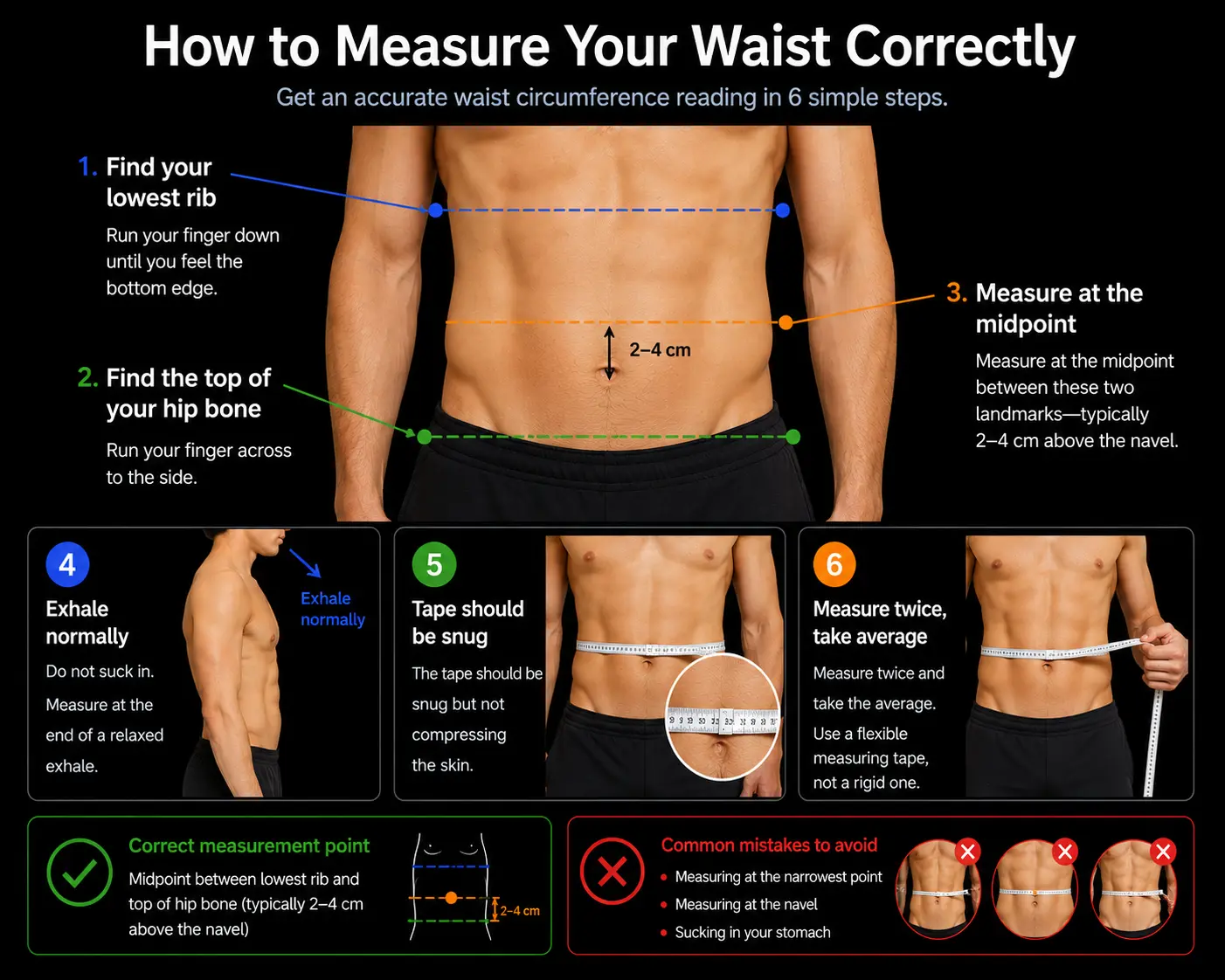
How to measure your waist correctly
This matters. Waist circumference is often measured wrong — people measure at the narrowest point (which flatters the number) or at the belly button (which is inconsistent across body types).
- Find your lowest rib. Run your finger down until you feel the bottom edge.
- Find the top of your hip bone (iliac crest). Run your finger across to the side.
- Measure at the midpoint between these two landmarks — typically 2–4 cm above the navel.
- Exhale normally. Do not suck in. Measure at the end of a relaxed exhale.
- The tape should be snug but not compressing the skin.
Measure twice and take the average. Use a flexible measuring tape, not a rigid one.
Personal take
I measured myself before I finished building the tool. I already knew the number wasn't going to be good. What I didn't expect was how wrong I'd been measuring for years before I actually looked up the correct method. The midpoint between the lowest rib and the iliac crest gives a completely different result from the narrowest point of the torso — which is what most people measure, including me. One is a real number. The other is flattery.
Reading your result
InResRisk calculates your WHtR and places you on a scale from Very Lean to High Risk. It also shows you exactly how far your waist is from the 0.5 threshold — in centimeters — so you know the concrete target, not just a vague category.
TRY INRESRISK
Two measurements. Thirty seconds. No account needed. Find out your insulin resistance risk score now.
OPEN INRESRISK →WHAT TO DO WITH YOUR RESULT
InResRisk gives you a number. What you do with it is up to you. Here's what the research says about each category.
WHtR below 0.5 — low to healthy range
You're below the elevated-risk threshold. That doesn't mean you're metabolically perfect, but your central adiposity isn't the primary risk driver. Focus on maintaining your waist, consistent sleep, and keeping processed food low.
WHtR 0.50–0.59 — elevated risk
This range is where most people are, and where most of the preventable damage accumulates over decades. The good news: it's highly reversible. A 5–10% reduction in body weight — concentrated in the waist — typically produces significant improvements in insulin sensitivity. Resistance training accelerates this by increasing muscle glucose uptake independently of insulin.
This is also the range where asking your doctor for a fasting insulin test is warranted. If your fasting insulin is above 10 µIU/mL alongside a WHtR above 0.5, you have meaningful evidence of insulin resistance.
WHtR 0.60 or above — high risk
At this level, visceral fat accumulation is severe enough that most people have measurable metabolic impairment. This warrants a conversation with a doctor and a full metabolic panel including HbA1c, fasting insulin, and lipids. The lifestyle interventions that work are the same, but they need to start now — not after you "see how things go."
FREQUENTLY ASKED QUESTIONS
Am I insulin resistant if my blood sugar is normal?
Possibly. Fasting glucose stays normal for years while insulin resistance develops. In many people, fasting insulin rises long before fasting glucose becomes abnormal. A normal fasting glucose with a WHtR above 0.5 is a common profile for people in the early stages of insulin resistance. Ask your doctor for a fasting insulin test, or request an oral glucose tolerance test (OGTT) if you want a more complete picture.
Personal take
This is the part that bothers me most about standard care. Where I live, fasting insulin is included in routine blood panels automatically — it's just part of the standard workup. That isn't true everywhere. In many countries, neither fasting insulin nor HbA1c is routine; you have to know to ask for it. Most people don't. The WHtR threshold exists precisely because of that gap — it gives you a usable signal without needing to navigate the healthcare system first.
What is a good waist-to-height ratio?
Below 0.5 is the generally accepted healthy threshold — your waist should be less than half your height. Below 0.4 is very lean. Between 0.5 and 0.6 is elevated risk. Above 0.6 is high risk. This threshold was validated across multiple large population studies and holds across different ethnicities, though some research suggests the threshold may be lower (around 0.47) for populations of Asian descent.
Is WHtR the same as waist-to-hip ratio?
No. Waist-to-hip ratio (WHR) compares your waist to your hip circumference. WHtR compares your waist to your height. WHtR requires only two measurements instead of three and has a single universal threshold (0.5) that doesn't vary by sex — unlike WHR, which uses different cut-offs for men and women. Research shows WHtR and WHR perform similarly as predictors of metabolic risk, but WHtR is simpler to measure and interpret.
Can I reduce my waist-to-height ratio?
Yes — and visceral fat is actually more responsive to intervention than subcutaneous fat (the fat you can pinch). The most effective approaches are: calorie restriction to produce a modest deficit (500–750 kcal/day), resistance training to increase muscle mass and insulin sensitivity, and reducing processed carbohydrates and ultra-processed foods. Studies consistently show that even a 5–7% reduction in body weight reduces visceral fat disproportionately — often by 10–20%.
Is waist-to-height ratio better than BMI for insulin resistance?
Yes, according to multiple large studies. BMI doesn't distinguish fat from muscle, and it ignores fat distribution. Visceral fat — the kind wrapped around your organs — is the metabolically active driver of insulin resistance, and it concentrates in the waist. WHtR directly captures this. A 2022 meta-analysis of over 300,000 participants confirmed that WHtR outperformed BMI and waist-to-hip ratio for predicting type 2 diabetes and cardiovascular disease.
What are the early signs of insulin resistance?
Early insulin resistance is often asymptomatic. When symptoms are present, they can include: fatigue after carbohydrate-heavy meals, difficulty losing weight despite caloric restriction, cravings for sugar and processed carbs, brain fog, skin tags (especially around the neck and armpits), and dark patches of skin called acanthosis nigricans. An elevated WHtR combined with any of these symptoms is a strong signal worth investigating with a doctor.